This is a SEO version of Journal of Laser Dentistry 1. Click here to view full version
« Previous Page Table of Contents Next Page »check-ups should be determined specifically for each patient between every 3 to 24 months.
Nonetheless, the continued stabilization of a patient's periodontal state depends largely, if not primarily, on the patient's oral hygiene at home as well as on the go. Without daily oral hygiene, periodontal disease will not be overcome, especially if the patient has a history of extensive periodontal disease.
Periodontal disease and tooth loss are associated with an increased risk of cancer.
A contributing cause may be low selenium in the diet: "Results showed that selenium has the strongest association with gum disease, with low levels increasing the risk by 13 fold."
Management
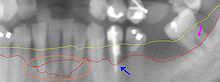
This section from a panoramic X-ray film depicts the teeth of the lower left quadrant, exhibiting generalized severe bone loss of 30– 80%. The red line depicts the existing bone level, whereas the yellow line depicts where the gingiva was originally (1–2 mm above the bone), prior to the patient developing periodontal disease. The pink arrow , on the right, points to a furcation involvement , or the loss of enough bone to reveal the location at which the individual roots of a molar begin to branch from the single root trunk; this is a sign of advanced periodontal disease. The
blue arrow , in the middle, shows up to 80% bone loss on tooth #21, and clinically, this tooth exhibited gross mobility. Finally, the
peach oval , to the left, highlights the aggressive nature with which periodontal disease generally affects mandibular incisors.
Because their roots are generally situated very close to each other, with minimal interproximal bone, and because of their location in the mouth, where plaque and calculus accumulation is greatest because of the pooling of saliva, mandibular anteriors suffer excessively. The split in the red line depicts varying densities of bone that contribute to a vague region of definitive bone height.
The cornerstone of successful periodontal treatment starts with establishing excellent oral hygiene. This includes twice daily brushing with daily flossing. Also the use of an interdental brush (called a Proxi-brush) is helpful if space between the teeth allows. Persons with dexterity problems such as arthritis may find oral hygiene to be difficult and may require more frequent professional care and/or the use of a powered tooth brush. Persons with periodontitis must realize that it is a chronic inflammatory disease and a lifelong regimen of excellent hygiene and professional maintenance care with a dentist/hygienist or periodontist is required to maintain affected teeth.
Initial therapy
Removal of microbic plaque and calculus is necessary to establish periodontal health. The first step in the treatment of periodontitis involves non-surgical cleaning below the gumline with a procedure called scaling and debridement. In the past, Root Planing was used (removal of cemental layer as well as calculus). This procedure involves use of specialized curettes to mechanically remove plaque and calculus from below the gumline, and may require multiple visits and local anesthesia to adequately complete. In addition to initial scaling and root planing, it may also be necessary to adjust the occlusion (bite) to prevent excessive force on teeth that have reduced bone support. Also it may be necessary to complete any other dental needs such as replacement of rough, plaque retentive restorations, closure of open contacts between teeth, and any other
This is a SEO version of Journal of Laser Dentistry 1. Click here to view full version
« Previous Page Table of Contents Next Page »